Project description
Conceptualisation
Multidimensional child growth has been conceptualised as:
“The process of continuous physical, psychological, and social change that builds a child's capacities to maximize life chances at the individual and societal level” - IUNS Task Force workshop, International Conference on Nutrition, Granada, 2013.
The approach is grounded in theories from different disciplines, such as nutrition transition theory from demography, parent-offspring conflict theory life history theory from evolutionary biology (Haisma, Yousefzadeh & Boele van Hensbroek, 2018).
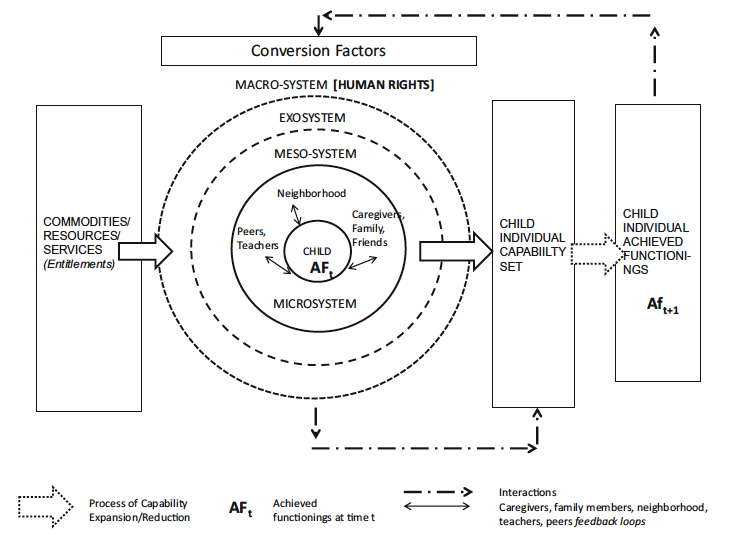
Building on Biggeri's conceptual model for child wellbeing (Biggeri and Karkara, 2014) and Bronferbrenner's ecological model (Bronferbrenner, 1994), we developed the Capability Framework for Child Growth. Following Nussbaum and Biggeri, we further adopted a rights-based approach to identify the dimensions for child growth (Yousefzadeh et al, 2019).
Publications
-
Haisma H, Yousefzadeh S, Boele P. (2018). Towards a Capability Approach to Child Growth: A theoretical framework. Maternal and Child Nutrition e12534.
-
Yousefzadeh S, Biggeri M, Arciprete C, Haisma H. (2019). A Capability Approach to Child Growth. Child Indicators Research, 12 (2), 711-731.
Qualitative work
To identify and understand the meaning of capabilities for child growth, we conducted qualitative research in Tanzania and in Bangladesh.

An ethnography of child growth: Socio-cultural context and meanings attached to child growth in Southeastern Tanzania
PhD thesis by Zaina Mchome at NIMR, Tanzania.
Main research questions
-
How does the socio-cultural context inform parents' framing of and practices around child growth?
-
What are contextual factors underlying capabilities for healthy child growth?
Main findings
Caregivers use multiple cultural markers for ascertaining healthy growth, including ‘being bonge’ (chubby), ‘being free of illness’, ‘eating well’, ‘growing in height’, as well as ‘having good kilos’ (weight). Despite the integration of some biomedical concepts into the local conceptualization of growth, the meanings attached to these concepts are largely rooted in the participants’ cultural framework. There exists a conceptual difference between the meanings attached to height from a biomedical and a local perspective. Whereas from a biomedical perspective the height increment is considered an outcome of growth, the caregivers did not see height as linked to nutrition, health, or overall growth. They referred to short stature as a normal condition that caregivers cannot influence; that is, as a function of God's will and/or heredity. While acknowledging short stature as an indicator of stunting, participants said it is not reliable. A number of cultural markers of stunting beyond height were mentioned. If these signs were not present, a child could not be regarded as stunted based on short stature only.
The study revealed inadequate knowledge about the aetiology of poor child growth, whereby parental non-adherence to postpartum sexual abstinence norms was a dominant cultural explanation for poor growth and development in a child. In case sexual abstinence is not maintained or when a mother conceives while still lactating, caregivers would wean their infants abruptly and completely to prevent poor growth. These findings imply that as biomedical experts, we need to understand how caregivers assign meaning to the growth of their children, and to take such meaning-giving into account when designing and implementing interventions aimed at promoting child growth and development.
Furthermore, the mothers’ capability to feed children was challenged by being overburdened by farm and domestic work and gendered patterns in childcare. Patriarchal cultural norms restricted women’s control of farm products and decision-making on household purchases. Which implies that a paradigm shift in Child Growth Monitoring (CGM) to a multi-dimensional approach that also includes the contextual information of an individual child and her/his caregivers is needed.
For more information, please see her PhD thesis and publications below.


Quote from mother's in-depth interview:
“We usually go to farms early in the morning and return home at 2.00 p.m. At times, we even lack a chance to eat lunch. You only come to get ugali (stiff porridge) in the evening, around 4:00 p.m. That is the only meal you have for the day. While working in the farm, you are starving, but the baby breastfeeds on you the whole day. Thus, both you and the baby starve. When I breastfeed, it feels as if my soul leaves the body. So, you say, aah, it is better to stop breastfeeding or to introduce food to him/her early so that s/he does not heavily breastfeed on you.” (KII-#03-TBA)
Publications
-
Mchome Z, Bailey A, Darak S, Kessy F, Haisma H. "He usually has what we call normal fevers": Cultural perspectives on healthy child growth in rural Southeastern Tanzania: An ethnographic enquiry. PLoS ONE, 14 (9).
-
Mchome ZS, Bailey A, Darak S, Haisma H. A child may be tall but also stunted. Conceptualisations of and meanings attached to childhood height and short stature in rural Tanzania. Maternal and Child Nutrition.
-
Mchome Zaina, Yousefzadeh Sepideh, Bailey Ajay, Haisma Hinke. (2020) “When I breastfeed, it feels as if my soul leaves the body”: Maternal capabilities for healthy child growth in rural Southeastern Tanzania. Int. J. Environ. Res. Public Health 17 (17), 6215.
-
Mchome Zaina, Bailey Ajay, Kessy Flora, Darak Shrinivas, Haisma Hinke (2020). Postpartum sex taboos and child growth in Tanzania: implications for child care. Maternal and Child Nutrition.
-
Mchome, Zaina Shabani. (2021). An ethnography of child growth. Socio-cultural context and meanings attached to child growth in Southeastern Tanzania. PhD thesis. University of Groningen.
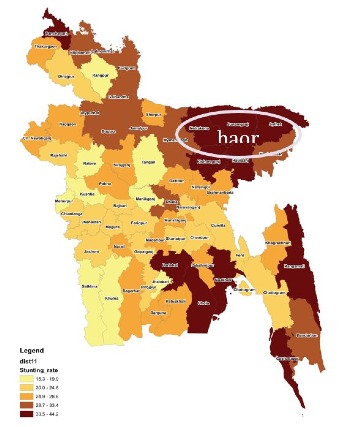
Saving the future in the swamp: A capability approach to child growth in haor areas of Bangladesh
PhD thesis by Barnali (Chumki) Chakraborty at BRAC James P Grant School of Public Health, BRAC University.
The objectives of her project were:
-
Review the work of other scholars who operationalised the capability approach to identify capabilities for different areas of wellbeing and human development. The key aim here is to take lessons from their work to build the methodology for our study in order to pioneer the application of the capability approach in the area of child growth.
-
Operationalise the capability approach in the area of child growth.
a. Identify a list of capabilities for child growth in the haor areas of Bangladesh.
b. Identify the contextual factors that underlie a capability of a parent to achieve any specific dimension of a child growth outcome. -
Identify the methodology for translating the concept of capabilities for child growth at the community level, and analyse the responses of community members in drawing up a contextualised list of capabilities.
Main findings
The study generated insights based on the findings of a narrative review of capability studies and participatory research done with the communities in haor areas. The key findings highlighted a set of capabilities for child growth at the level of the child, the mother, the father, and the household built on the emic perspectives of the parents in haor, which indicated the deprivations of multidimensional capabilities that are relevant for child growth in haor. Maternal and child survival was found to be at the core of the concept of child growth in the haor context, which is a collective goal to be achieved by the haor communities. Mothers lack the autonomy to seek health care by themselves because they have insufficient access to financial resources, or to women-friendly social arrangements for health care after a caesarean delivery. Their limited knowledge about how to find the location of the health facility, and their gendered roles restricting them to indoor activities, made the fathers responsible for ensuring the survival of their family members. This is expressed by them as their capability “to save the future”.
The study highlighted the importance of addressing the socially constructed gendered differences in order to improve women’s autonomy and to engage with the parents regarding their shared responsibilities. Finally, the study demonstrated how capabilities can be identified in a democratic or participatory way by providing an example of how doxastic and epistemic approaches can be combined in the process of the co-creation of knowledge by the participants and the researchers.
In addition to her qualitative work, she also developed a survey questionnaire on child growth from a capability perspective. This survey is freely available upon request to Barnali (email: barnali.chakraborty bracu.ac.bd).




Quote from fathers:
“See, before the marriage people dream of having a beautiful wife, then after getting married people dream of having babies. (Someone starts laughing). No do not laugh! Why do you laugh? When we talk about the important aspects of marriage you laugh! See these children are our future. Now to get this future, if the future along with the person through whom the future is delivered die, it takes us through the saddest experience of life. The saddest thing more than anything!” FGD, Fathers, Golbogi, Baniachang.
Publications
-
Chakraborty Barnali. (2022). Saving the Future in the Swamp: a Capability Approach to Child Growth in haor areas of Bangladesh. University of Groningen. https://doi.org/10.33612/diss.222295474
-
Chakraborty, B.; Darak, S.; Haisma, H. (2020) Maternal and Child Survival in Haor Region in Bangladesh. An Analysis of Fathers’ Capabilities to Save the Future. Int. J. Environ. Res. Public Health, 17(16), 5781.
-
Chakraborty Barnali, Yousefzadeh Sepideh, Darak Shrinivas, and Haisma Hinke (2020). "We struggle with the earth everyday": parents' perspectives on the capabilities for healthy child growth in haor region of Bangladesh. BMC Public Health 20: 140.
Quantitative work
Developing the Multidimensional Index for Child Growth (MICG)
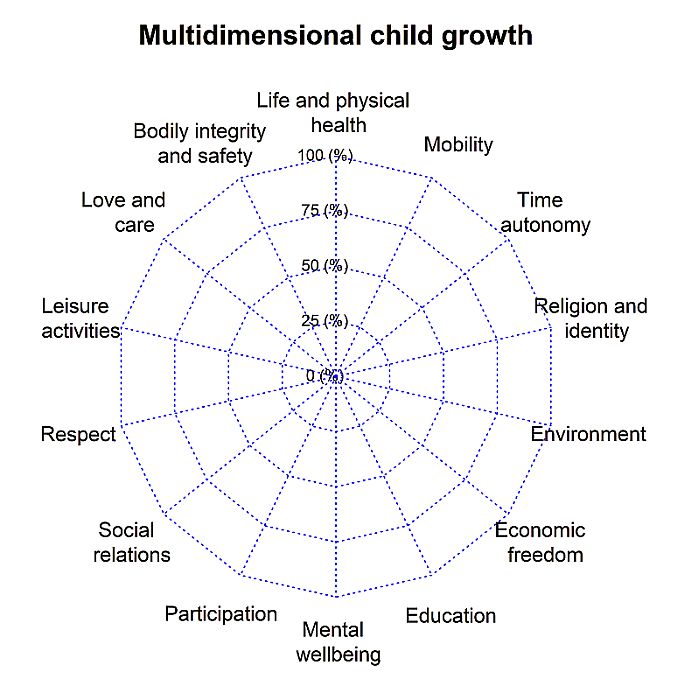
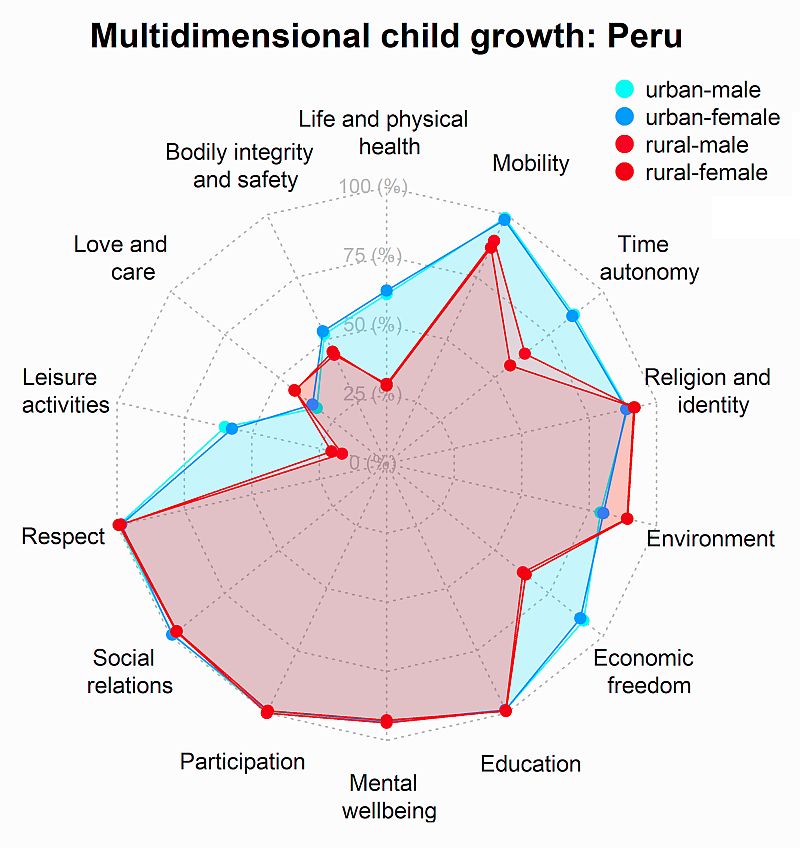
We used the spiderweb visualisation for the design of the MICG. The 14 dimensions reflect the dimensions as identified by Biggeri et al (2006) and are reflecting the Convention of the Rights of the Child.
Using the MICG for comparisons between countries
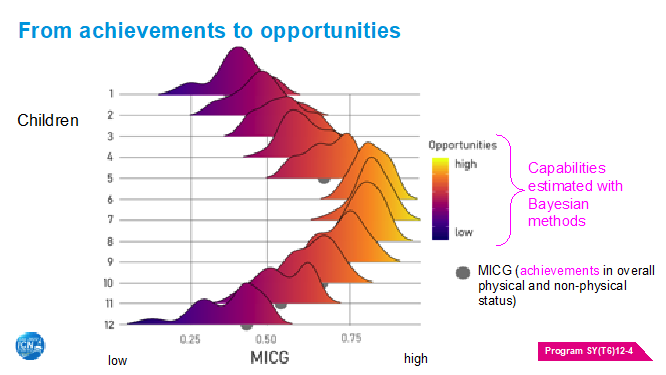
A Multidimensional Index of Child Growth (MICG) was calculated to identify physical and non-physical deprivations experienced by 5-year-old children living in Ethiopia, Vietnam, India, and Peru. A Bayesian extension of the MICG was applied to identify specific children, at individual level, who are most likely to be left behind or neglected by social and health development policies. As children’s opportunities and achievements depend on parental attitudes and the children’s environment, these are included as part of the MICG indicators.
The MICG measures the achievements of children with observed indicators. Achievements are equal to the observed situation of children. To measure the opportunities available to children—this is, their potential child growth above or below their achievements—, Bayesian stochastic frontier analysis was applied to the MICG. The Bayesian model estimates potential alternative values of multidimensional child growth that could be negatively or positively affected by children’s observed characteristics. We chose to use geographical location and sex as discriminating characteristics, besides random circumstances that affect the achievements measured by the MICG. Specific children that could be left behind are those with the lowest opportunities for physical and non-physical growth; this is, those children that have the lowest estimated values of the potential MICG.
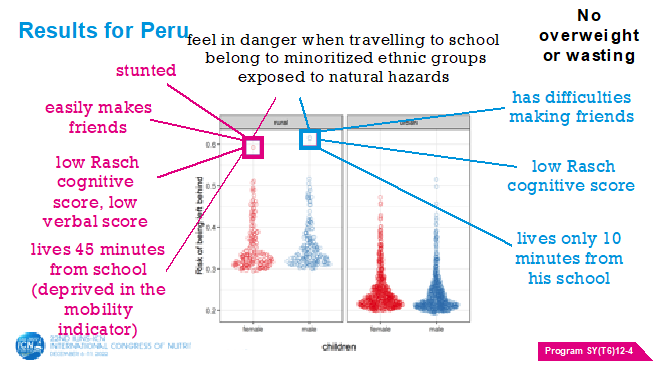
In all countries, child labor and physical growth were found to be worse in rural areas compared to urban areas, but non-physical deprivations related to leisure time and cognitive and verbal development are country specific. To illustrate how the Bayesian analysis helps us get a deeper insight into inequalities, we identified two children from Peru (one of each sex) who have the highest risk of being left behind in their process of multidimensional growth. In the physical dimension, no children were overweight or wasting; however, the girl is stunted while the boy is not. In the non-physical dimensions, both children feel in danger when travelling to school and their parents believe that the special feeling of love between parent and child is only moderately important. At the level of the children's opportunities, the little girl can easily make friends with other children, but the boy has difficulties making friends with other children. Both children have a Rasch cognitive score below the first quintile, but the girl also has a score in the verbal PPVT below the first quintile. Both children belong to minoritized ethnic groups and have low time for leisure as they help in domestic tasks. Finally, both children are exposed to environmental risks related to natural hazards, and while the boy lives only 10 minutes from his school, the girl lives 45 minutes from school, hence suggesting that she may be deprived in terms of mobility. The evidence of our multi-dimensional approach indicates that a focus on opportunities rather than achievements can identify hidden inequalities and hence guide context-specific interventions."
Publications
-
Gonzales Martinez, R., Wells, J., Anand, P., Pelto, G. Dhansay, M.A., Haisma, H. Community participation and multi-dimensional child growth: evidence from the Vietnam Young Lives Study. Current developments in nutrition Mar 17;6(4).
Policy and practice
Haisma Hinke, Pelto Gretel, Venkatapuram Sridhar, Yousefzadeh Sepideh, Kramer Lybrich, members of the Working Group "Towards a multi-dimensional index of child growth". (2020) Towards a multi-dimensional index of child growth to combat the double burden of malnutrition. Annals Nutrition Metabolism; 75:123–126.
| Last modified: | 24 February 2025 1.33 p.m. |